| |

|
This state of affairs gives rise to the following paradox in the ICU. Namely, to watch over the patient, the hospital workers eject from the ICU the family -- who are watching over the patient. This is because the hospital workers are concentrating only on the medical aspect of the patient. [30/31] Apart from the few minutes twice a day when they can be face to face with the patient, the family can only wait outside the ICU. Compared to the all-pervasive medical line of sight of the nurses, and monitoring machines, the family’s “line of sight” to the patient inside the ICU is blocked. Only the medical aspect of the patient is watched seriously, and this unique, uniform gaze is all that fills the ICU.
Treatment in the ICU is said to be comprehensive treatment that treats the whole human body. However, just when the human body should be seen comprehensively, in fact, the “human” is seen only one-sidedly, with all other aspects excluded to the utmost extent. I think this is the largest paradox of the ICU. Why does this paradox exist? It is because looking at patients in this way is thought to be tremendously efficient. In an efficient place, medical treatment can bring its full power to bear. Modern medicine is efficient medicine.
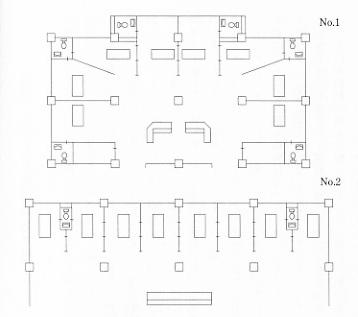
The problem of “line of sight” in the ICU is made clearer if you take a look at figure 3 (ICUKango Nyuumon p.131). This is the layout of an ICU that has been divided into private rooms. The beds have been separated with walls or curtains between them. Fellow patients have had their lines of sight entirely cut off. However, it has been made possible to see all of the patients from the nurses’ station in the very center. Here the intense gaze of those supervising falls on all those being supervised. This one central watchtower is designed to allow supervision of many small rooms from one place.
This looks incredibly similar to the structure of the modern European thinker Jeremy Bentham’s “Panopticon” -- a design for a prison. This was designed so that all the movements of the inmates could be seen from a central watchtower. [31/32] The ICU is at the forefront of contemporary medicine, which started in Europe, and so it is of deep significance that the model of the Panopticon reappears here. Perhaps only a modern gaze fills the ICU.
The problem of a brain dead person occupying a bed
So let us suppose that, despite the strenuous medical efforts within the ICU, a patient becomes a brain dead person. This is also a defeat of the ICU’s medical treatment. Considering contemporary medical treatment, we can’t expect brain dead patients to recover. We can only wait for their hearts to stop.
A brain dead person is lying on a bed in an ICU. Their heart continues to beat normally for several days, and during this time, they must occupy a bed. This is the cause of many problems.
For how long should medical treatment continue?
The first problem that arises is that of when to cease artificial respiration. It’s acceptable to discontinue artificial respiration if the heart stops within two or three days, but what should we do if the heart continues to beat for a week or more? If we discontinue artificial respiration, then a brain dead person’s heart will soon stop beating. It seems to be particularly true that in cases where a brain dead person is still young, their family expresses the wish that the patient remains as they are until their heart stops beating naturally. As far as the circumstances permit, the family’s wishes should be respected, but the issue is not that simple. [32/33]
Firstly, if a brain dead person is continually occupying a bed, there is the danger that in an emergency, an emergency patient cannot be admitted to the hospital. Also, to regulate and maintain an artificial respirator takes a lot of labour. There is also the way of thinking that if a lot of labour is being spent on patients who won’t recover, it should really be spent on patients who have a chance of recovery. To run an artificial respiration machine of course takes a lot of money. This expense is sometimes paid by health insurance, and sometimes by the hospital. Payment by health insurance means it is paid for by our insurance premiums or taxes. There is the feeling that using public money on brain dead patients who have no chance of recovery is just throwing it away. Finally there is the opinion that keeping a brain dead person who has no chance of recovery on an artificial respirator is disrespectful to them as human beings.
The continuous treatment of a brain dead patient is not limited to the use of artificial respiration machines. First and foremost there is medication to boost blood pressure, as well as various other medications supplied by intravenous tubes. Similarly, nutrients to keep the brain dead patient’s body alive are also supplied in liquid form. In some cases it is necessary to perform a blood transfusion. These kinds of medical treatments consume labour and money. And on top of that, there is a chronic shortage of blood for blood transfusions. There is the opinion that using valuable blood on brain dead patients who will not recover is just immoral.
How long should nursing continue?
As stated in chapter one, brain dead patients require various kinds of care. [33/34] For how long should we continue to measure and record the temperature, pulse and blood pressure of a person who has no hope of recovery? For how long should we clean a brain dead person’s body for them? If nurses are tied up with this kind of continuous care, it could possibly hinder the care of other patients. Nurses might also become disheartened by the futility of having to give continuous care to a patient who will never recover.
To supervise brain dead people properly requires many kinds of care. It takes about as much trouble and labour as for a patient in a coma. This point has rarely been given much weight in literature about brain dead people. Here I will try to introduce in a more concrete way the kind and level of care that is necessary to supervise both a brain dead person and a person in a coma, as it is the same.
First, the inside of their mouth is cleaned regularly. Because the patient’s mouth dries out easily and is not very moist, it becomes easy for bacteria to breed. So using a cotton swab, the upper and lower teeth and gums, the tongue and the inside of the mouth are painstakingly cleaned.
The body is wiped clean. If the skin is not kept clean, then rashes can break out, and it becomes difficult for the body to perspire freely. In particular, if the genital area containing the tube used to pass urine is not kept clean, it may become inflamed. The patient’s hair is washed with medicinal alcohol. The eyes, nose and ears easily become dirty and so are cleaned with an oiled cotton swab. Because patients in a coma often have their eyes slightly open, their eyes are covered with bandages to prevent the cornea drying out.
The position of the body is changed. The patient is lying on the bed, connected to various tubes, and facing upwards in a fixed position. If they were to be left in this position, then the side of their body with the weight on it would develop bed sores. [34/35] So the position of their body is changed every two to three hours. This takes more than two people who turn the body in an instant. At the same time, massage and shiatsu is used to relieve the muscles. Because the patients cannot move themselves, the nurses exercise the joints of the legs, knees, thighs, and the shoulders at regular intervals.
The patients have intravenous and blood transfusion tubes inserted in them. The skin is checked thoroughly and often, to make sure that the needles are inserted correctly, and that the skin has not become inflamed. A check is made on the amount of the drip.
Urine and bowl movements are disposed of. Urine comes out through a tube, so the amount of urine is measured.
Even supposing that a person is brain dead, if they are to be supervised correctly, then this amount of nursing is necessary to keep their heart beating. This is quite a burden. It wouldn’t be a strange thing if, when wiping down the patients’ bodies and changing their position, some feelings of doubt might arise in a nurse.
Funding treatment and providing insurance for brain dead people
If you support a brain dead person in the ICU, it takes a certain amount of labor, medical resources and expenses. For example, according to Yusuke Sawada, costs for one week of IVH (high calorie drip), artificial respiration and care comes to:
- 2 official diagnoses of brain death: 100,000yen
- One week of examination in the ICU: 180,000yen [35/36]
- Nutrient supplies, oxygen supply, medications, blood plasma, expenses for antibiotics: 580,000yen
- Heart massage, death formalities: 80,000yen
- Miscellaneous costs: 30,000yen
Total:1,060,000yen (around USD $10,000)
Sawada says the following:
If a person receives care for 50 days after being pronounced brain dead, then including costs for dealing with the dead body, the total comes to approximately 6 million yen. The patient is liable for around 30,000yen and so in reality insurance pays up around 6-7 million yen for the care of the brain dead person’s body. (Zokuzoku Nosushi to Shinzoushi no Aida de (Between Heart and Brain Death Part 3.)), Medical Friend, The Japan Society for Transplantation (ed.) Sep. 1986, pp. 219-221.)
So it’s not strange to hear medical staff calling for treatment and care for brain dead patients to be cut off as soon as possible. For example, KagoshimaUniversity hospital has set forth a policy to end application of antibiotics, blood pressure medication, dialysis and so on, even without the agreement of the patient’s family. The family’s agreement is required for the withdrawal of artificial respiration.
These calls do not just come from the medical field. The same appeals can be heard from those thinking about national medical economics. For example, Shin’ichi Fujita, a member of the Asahi Shimbun group has this to say:
Once a person has been medically certified as brain dead, even though the respirator is moving and the heart continues to beat, it’s not to keep the patient alive but to console the family, and this is widely known. [36/37]
This is nothing to do with the “life” of the patient, but nothing more than wasteful playing with the “dead body” of the patient, and sooner or later, I think that the general population will come to see the common sense of this.
(…statement partially omitted…)
If a patient is judged to be brain dead, with a zero percent chance of his or her life being saved, then what cause does it serve to keep the respirator running for a day, two days or even a week, just because the family wishes it so?
I think it’s just for appearances.
Of course, to let go of a dead person, a certain amount of time is necessary; that goes without saying. However, just because of that, there is no logic to the idea that the dead body should be cared for indefinitely even after the medical diagnosis of “death,” just to let go of the dead person. After one week, the brain begins to liquify itself, and the smell of death is unbearable, I have heard. It seems that some people just do not wish to see the death of a blood relative.
However, if the blood relatives were to look from the standpoint of the dead person, they would understand that to have all sorts of tubes and needles continually inserted into you, so your body is toyed around with for no good reason is a terrible annoyance and amounts to desecration. I have heard that in any hospital, the lowest cost for maintaining a body after brain death for one day is 50,000yen. In some hospitals one day costs more than 100,000yen. If claimed as “medical expenses,” this whole cost is paid as part of health insurance, and this is a problem. [37/38]
Sooner or later we may have to draw the line. If brain death has been diagnosed, then because medical treatment stops (a dead person cannot be treated), I think there is no other choice but for families who wish the respirator to continue running anyway to shoulder the medical expenses themselves. How many people would really want to continue the maintenance of a dead body at 50,000yen or even 100,000yen per day? If, faced with these kinds of costs, a family says, “Please stop medical treatment” then there is really nothing more we should say to them.” (Seiji to Seimeirinri (Politics and Bioethics)), FA, Diet Members’ Bioethics Research League (ed.), Feb. 1985, pp.29-31.)
In the final report of the Japan Medical Association’s Bioethics Committee (Jan.12, 1988), there is the following passage:
In the case of organ donation, medicinal and blood transfusion measures continue after the pronouncement of brain death, as well as artificial respiration. It should be examined whether or not the application of medical insurance is the best way to deal with the problem of medical expenses occurring in the case stated above.
There is no doubt that the problem of medical insurance will become a matter for social debate.
What is the best way to treat and nurse a brain dead person?
Due to the above circumstances, the first ethical problem of brain death, that is to say, the first ethical problem of the ICU arises. Let’s review it once again. The ethical problem of brain death was, what is the best way to proceed with the person to person relationships surrounding brain dead people? In the same way, the ethical problem of the ICU is, what is the best way to proceed concerning brain dead people within the place just described known as the ICU? [38/39]
The ethical problems in the ICU can be organised into roughly three types.
1) Is it right to cut off medical treatment and nursing, and artificially accelerate the heart failure of a brain dead person?
2) Who should decide this?
3) What should we do if the family wants medical treatment and nursing for the brain dead person to continue?
These are difficult problems that do not have a simple answer. There are many possible ways of thinking about it. I think that if the brain dead person has expressed the desire at some point, and if his or her family consents, then we should respect a request to terminate medical treatment and care. However, there is one condition. This is as follows: the decision to stop medical treatment should be made by the doctor in charge who has fully confirmed the patient’s former wishes and the family’s will. When the family wish for medical treatment and nursing to continue, the nurses and doctors, should continue for as long as possible, providing as much care as they can for the family of the brain dead person.
I will try to state this point in a more easily understandable way.
I think there are two ways of thinking concerning the grounds for the opinion that we should stop medical treatment and nursing of brain dead people. The first is that, although of course we want to keep a brain dead person’s heart alive, if we consider the labour of the doctors and nurses, and the hindrance to other patients in the ICU, and the expenditure of essential resources, and money, then we should end medical treatment and nursing. In other words, this opinion is that although there may be reasons for giving brain dead people medical treatment and nursing, if we consider the surrounding circumstances, this is not a good enough reason to continue treatment. I think that this argument is correct, if you think we should concentrate only on how to distribute scarce medical resources. [39/40]
The other way of thinking is that we should end medical treatment and nursing of brain dead people because it is futile. Brain dead people are not going to recover. Giving them medical treatment and nursing is a complete waste, and therefore a meaningless action. The Japan Medical Association too, holds that as brain dead people are medically dead, then treatment of the dead body cannot be said to be medical treatment. This is their way of thinking. I think that this is mistaken.
The reason for this is because, I think that the medical care of the dead body can be said to be excellent medical treatment. Using the phrase “dead body” here might suggest that I am thinking of the brain dead person only as a dead body, so to avoid this misunderstanding, I would like to rephrase my last sentence to the following: I think that the medical care of brain dead people can be said to be excellent medical care.
Many people will probably have a strange impression as they read this. “There is no such thing as medical care for brain dead people. You see, brain dead people are already medically dead, and won’t recover, and aren’t even conscious. What kind of treatment are you going to give them? What kind of merit do you see in such treatment?”
To those who think in this way -- you are already caught in a trap. This is the trap of thinking that you can understand brain death just by understanding the contents of the brain, as stated in chapter 1.
You must change your way of thinking.
Let’s return and consider the issue from the beginning. “Brain death” did not concern the contents of the brain, but rather person to person relationships. “Brain death” was about the human relationships surrounding the brain dead person. What I mean is, the medical care of a brain dead person is medical care of the “sphere” of the human relationships surrounding the brain dead person. [40/41]
Well, what could “medical care of the sphere” be?
The life saving treatment in the ICU was medical care that takes as its focus the treatment of the patient’s body and the inside of the patient’s brain. By contrast, I want to define “care of the sphere” as medical treatment that takes as its focus the work that supports and cares for the condition of the human relationships that surround the patient.
Medical treatment that centers around care of the sphere of person to person relationships
Let’s take a more concrete look at the medical care of this sphere.
When a comatose patient is carried into the ICU for the first time, the first thing that occurs is “life saving treatment of the comatose patient.” This medical care concentrates completely on the contents of the patient’s brain, and their body. From the time when this treatment fails, and the patient becomes a brain dead person, then “treatment of the sphere” -- which is different from the life saving treatment of the patient -- begins. Or, in other words, we begin the “medical treatment of brain death.”
Amongst all the people surrounding the brain dead person receiving medical treatment, the most in need of assistance are the family of the brain dead person. As has already been stated before, the ICU is a world in which the attendant gaze of the blood relatives is excluded to the utmost extent. The family are continuously waiting outside the ICU, hoping to see the figure of their own kin recover and come out of the ICU, so to suddenly be told that “the patient is brain dead” leaves them at a loss for how they should react.
This is because the family cannot yet completely accept the death of their blood relative. At some point the brain dead person’s heart will stop and their dead body will become cold. [41/42] But until that point, the family do not fully comprehend that this will happen, and they have not said farewell to their loved one. This experience is necessary for a family to fully accept the death of a brain dead person. If you switch off the respirator and perform organ transplants before they can have this experience, then a perpetual scar will be left on the hearts of the family.
The family’s acceptance of their loss comes about through care of the blood relative who has become brain dead -- care or attendance of the brain dead person. The first job of the medical treatment of the brain dead person is helping the family to attend the brain dead person. Helping the family to attend the brain dead person means, establishing a quiet place away from doctors and nurses for the family attending the brain dead person, showing consideration, and in other words providing nursing care for the family.
The emergency treatment in the ICU was medical treatment that prioritised the medical health aspect of the patient above nursing the patient. By contrast, the medical treatment after brain death is medical treatment that places priority on the nursing care of the sphere of person to person relationships surrounding the brain dead person. In particular, the nursing care of the family watching over the brain dead person becomes the main focus here.
I think that the opinion that care of the family’s feelings is best left up to nurses, and that it does not deserve the name of “medical treatment” is due to the arrogance of doctors. This arrogance is the cause of a growing feeling of distrust of doctors by patients and families, as will be covered in the next chapter. By clinging to the fixed idea that medical treatment is to cure the bodies of people who have a chance of recovery, the treatment of brain dead people is ignored. If you are aware of the fact that the goal of medical treatment of a brain dead person is nursing care of the person to person sphere, you can easily come to understand the concept of medical treatment of brain death.
The ethical problem of the ICU was how best to proceed concerning the relationships of the family, doctors and nurses, surrounding the brain dead person in the ICU. [42/43] Now, we can give this question only one answer. It is that doctors and nurses should care for the family watching over the brain dead person. Therefore I think that our society should adopt the courtesy of caring for the family watching over the brain dead person.
This way of thinking is not entirely new in itself.
As a matter of fact, in the case of “terminal care” for cancer patients facing death, alongside the care of the patients themselves, the importance of caring for the patient’s family is also beginning to be discussed. The family, watching over the final struggle against illness by a blood relative with whom they have shared a long life, are in a state of confusion, pain and sadness. The care of the mental health of the family continues after the death of the patient, by making efforts to contact the family and staying with them in their time of sadness. (Ganshi Kea Manyuaru (Care Manual for Cancer Deaths)), Masahiro IIo and Hiroomi Kouno, Igaku Shoin, Apr.1987). In the case of “terminal care,” the family receives this kind of care. This is not simply an addition to life-prolonging medicine. Instead, at the bottom of terminal care lies “nursing care of the sphere” of human relationships that takes the family as one of its main objects. One characteristic of the essence of nursing is care of the person to person sphere. In the ICU, specific techniques concerning the brain dead patient’s body were given priority, but even here the “nursing care of the sphere” was by no means absent.
I want to call this medical treatment that centers around the “nursing care of the sphere”: “sphere treatment.” If “sphere” is too difficult a word, it can be expressed as “treatment of relations.”
The treatment for brain death is the same. We must move towards the existence of medical treatment that centers around care of the sphere. [43/44]
Caring for Brain Dead People
So, to support a family’s care of a brain dead person, doctors and nurses must do three things:
1) Guarantee a sufficient amount of time spent for the family to attend the brain dead person.
2) Offer to set up a quiet place where this can be done.
3) Offer basic minimum nursing care to a brain dead person.
The first two relate to the care of the family, and the third relates to the care of the brain dead person. I shall explain them in order.
The care of a brain dead person is care that allows the family to bid farewell and let go of the brain dead person, through realising that the brain dead person is at last a cold dead body that will not recover. In the case of a brain dead person, who is warm and with blood still flowing, it is significantly harder to say goodbye.
When attending a brain dead person, the (imminent) death takes a lot of time to accept. Those with a warm brain dead person before them cannot suddenly let go as if it were a cold dead body; they need more time. Even doctors too, such as Tateo Sugimoto speaks of his experience as follows:
We have reached a point these days where there is no system where doctors and patients and their families can speak on completely equal terms. If there is a sudden unexpected incident such as a traffic accident, no matter how simple the contents of the doctor’s explanation is, a certain amount of time is necessary before a level of acceptance is reached. Even from my standpoint, as a person who understands the physiology of the brain, it took several days for me to accept it satisfactorily. [44/45] Understanding the inside of the brain and actually comprehending it in reality are two separate things. (Kita Kamo Shirenai Seifuku (A Uniform My Son Might Have Worn), p.198).
A group formed by Yoshiko Taguchi, from Nippon Medical School, is conducting research that records in detail the mental condition of the brain dead person’s family (Asahi Shimbun 1988, Jan 26, morning edition). For example, the mental changes in the wife of a 52 year old brain dead man, were divided into four stages. The first stage lasted until 3 days after the diagnosis of brain death. It was a state of panic and incomprehension. The second stage was from the 3rd to the 4th day. This was a state of confusion and anxiety, and the family prayed for a miracle. The third stage was from the 4th to the 6th day. Their emotions become more ordered and they became able to think about things realistically. And when they reached the fourth stage, from the 6th to the 10th day, they finally accepted the death, and are able to ask for the respirator to be removed.
In the case of this family, from the diagnosis of brain death to acceptance of the death took a little over one week. I don’t know under what conditions and for what length of time the family were allowed to visit the brain dead person in this ICU, but to accept the death of a family member, I think that several days to one week is necessary as the minimum length of time.
Depending on the family, there are many levels to their acceptance of the death. For example, a level at which they understand it in their heads, but have not really registered it yet, a level at which patients’ sadness and confusion seems to have passed and they are comparatively calm, a level at which you have become able to assent to removing the respirator of your own free will, and the level at which you can finally accept in reality that the patient has passed away and calmly respond to the situation, and so on. It might take many months or even many years to reach this final state of mind, even after the patient’s heart has stopped beating. [45/46]
Although there are many levels to be distinguished during the acceptance of death, I would like to think now about the level that could be described as “Having passed the state of confusion and panic, and reaching a level at which you have become able to assent to removing the respirator of your own free will.”
By the above reasoning, to really assist in the care of brain dead people, the family must be guaranteed at least several days to one whole week. However, under the current system family members are not allowed into the ICU apart from about ten minutes twice a day, so I wonder if this guarantee is really possible. If only the hospital side would take an interest, it would not be impossible for the family to spend an extended amount of time in the ICU. Keiko Tajima says the following:
In America from the mid 1950’s to the 1960’s, the problem of “ICU syndrome” grew steadily worse, but one measure introduced to deal with it was to extend the visiting time of a family and break down the visiting restrictions, and it seems their condition began to improve.
The relation of long visits to equipment, medical treatment, and the level and frequency of care in the ICU must be considered, but if nurses make accurate judgements according to the necessity of these things, it’s possible to say that attending will not in any way obstruct medical care or nursing. I hope that in the management of future ICUs, visiting times will have as few restrictions as possible.” (ICUKango Nyuumon, pp. 32-33.)
So as long as the doctors and nurses do not resent it, isn’t it possible for the family to visit brain dead patients in the ICU for an extended period of time? Doubtless it will be said that there is the danger of the family bringing dust and bacteria into the ICU. But Tajima says, “There are modern ventilation systems and air purifiers, and if these are taken into account then surely this situation will improve.” (same publication, p.32.) [46/47] Further, because the patient is already brain dead, there is no need to be so nervous about the family causing the monitoring equipment attached to the patient to malfunction.
Let’s think about nursing care in relation to a brain dead person. The very first thing that should be done is to make it so that the family receives support in their attendance of the brain dead person. If the very least consideration is to be given to the attendance of the death of a person and the family’s acceptance of this death, then we must not neglect to pay respect to the dying (or dead) person’s body and to keep it clean. For example, at a funeral, the body is treated with great care and made so that it looks presentable and not offensive. On the occasion of a funeral, a parting, this happens as a matter of common sense.
The attendance of a brain dead person is the same. When they support the parting of the family from the brain dead person, I think that as a show of respect and courtesy to the family, doctors and nurses should keep care of the patient to a minimum. So it is not necessary to continue all the care that took place before the patient was pronounced brain dead. To be useful to the attendance of the family, only care that does not impinge on the dignity of a brain dead person should continue. For example, it’s acceptable to detach various types of monitoring equipment. It might also be acceptable in some cases to stop blood transfusion. The use of artificial respiration machines, intravenous tubes for nutrition, and various medicines including vasopressin should be kept to a minimum. The body’s position may still be changed, and it may be cleaned. The family members could participate in this care, not just the nurses. I think the exercising of the patient’s legs and arms can be left out. Exactly what should continue and what may stop should be decided by the nurses and doctors present at the time. [47/48]
Moving the bed outside the ICU
If we think in this way, the number of kinds of machines and equipment around the brain dead person will be drastically reduced. Further, as this is not a life and death situation, there is no need for such severe observation. And if we do that, then another possibility for attending to the brain dead person arises. It’s as you think. Move the bed right out of the ICU. The bed has wheels attached, so swap the artificial respirator for a smaller one, and taking along the IVH drip, move the bed right out of the ICU.
If the bed is put in an ordinary hospital room, then other patients may be disturbed, so an individual room would be fine. Depending on the size of the hospital, there is an even better method. Please take another look at the diagram 2 of the ICU at Kobe City General Hospital. There are many small rooms adjoining the main ICU. Amongst these, there is a family waiting room, a briefing room, a conference room, a doctor’s lounge and so on. One of these should be made into a room to attend the brain dead person. With a little juggling, this wouldn’t be impossible. In newly-established wards, rooms made especially for attending brain dead patients, between the ICU and ordinary wards, are being considered (a kind of “halfway-house” concept if you will). Of course, rooms for attending brain dead patients do not have to be permanently so; they may be used for other purposes according to the circumstances. Recently, in large hospitals, “serious illness supervision rooms,” lying directly between the ICU and ordinary hospital rooms have begun to appear. So for example, what if we section off a corner in this serious illness supervision room, and make it into a room for attending brain dead people? I think that it is worth considering. [48/49]
If you take a brain dead person out of the ICU, then obviously it will speed up heart failure. However, because treatment of a brain dead person is nursing those attending them rather than extending the life of their heart, then if the family so wishes, doctors need not have a guilty conscience about this.
Those who hold the opinion that medical treatment of brain dead people is useless medicine, also say that brain dead people should quickly be taken off respirators and moved out of the ICU. However, they are saying this only thinking of economic efficiency. The necessity of attending the brain dead person does not enter their field of view. This way of thinking should be ruled out.
The members at the Japan Medical Association’s Bioethics Committee made a statement at a press conference to the effect that keeping brain dead people on artificial respirators was contrary to respect for human beings. However, the wishes of the brain dead person made before the event should take priority, followed by the judgement of the family attending the brain dead person, so this is not a general proposal that should have been put forward by an authoritative group.
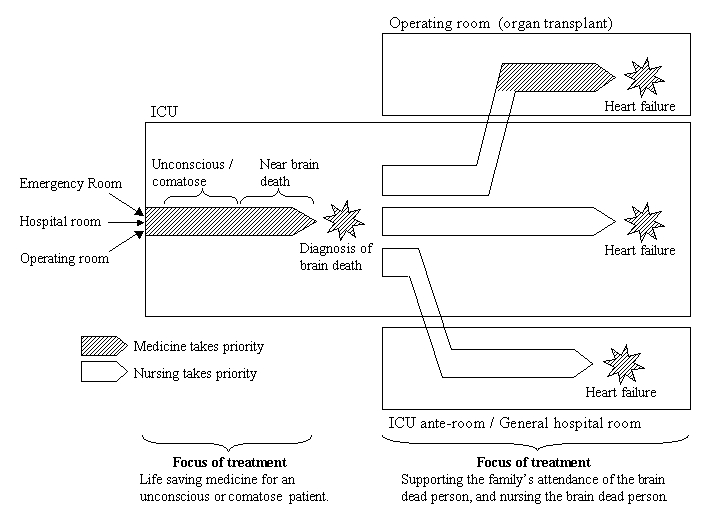
From life saving medicine to medicine centered around nursing
Well, let’s express what has been said so far as a diagram (refer to the following figure 4).
A patient who cannot regain consciousness or is in a comatose state is brought into the ICU. Life-saving treatment is given, but despite that, the patient falls into a state of brain death. The treatment that takes place at this time is first and foremost treatment for the patient in a comatose state. [49/50] The nurses provide necessary care for the body so that life-saving treatment may have its greatest effect. They also try to present easily understandable information to the family waiting outside the ICU. |